|
INDIA REPORT
Leprosy Control in India
A senior health official puts the elimination achievement in context
AUTHOR: Dr. G.P.S. Dhillon
| Dr. G.P.S. Dhillon is India's Deputy Director General of Health Service (Leprosy), Ministry of Health and Family Welfare. |
The first record of a leprosy-like disease in India appeared in the sixth century BC. It is said that leprosy was referred to as “Kusht” in Vedic writing, which is how the disease is known even to this day.
The government of India started a National Leprosy Control Program in 1955 based on Dapsone domiciliary treatment through vertical units implementing survey, education and treatment activities. The National Leprosy Eradication Program was launched in 1983 with the objective of arresting disease activity in all known cases of leprosy with the use of multidrug therapy.
In December 2005, at the end of some two decades of the fight against leprosy with MDT, India succeeded in achieving the goal of elimination of leprosy as a public health problem at the national level, reaching a prevalence rate of 0.95 per 10,000 population. Three months later, on March 31, 2006, PR was further reduced to 0.84.
India contributes nearly 70% of the global case load of leprosy and therefore this achievement will have a huge bearing on the global situation. The gradual reduction in newly detected leprosy cases since the year 2002-03 also speaks well of the strategy.
The significant achievements associated with leprosy elimination in India have been:
・changes in service delivery to the integrated system through the Primary Health Centers, which increased people's accessibility to services nearer to home;
・training and retraining of a large number of General Health Care practitioners to make them proficient in recognizing leprosy and providing health education;
・repeated mass awareness campaigns that havehelped to increase public awareness of leprosy and its curability, resulting in an increase in self-reporting for diagnosis and treatment;
・the slow but sure diminishing of stigma associated with the disease in society;
・streamlining of data generation, reporting and monitoring through a Simplified Information System (SIS) introduced in 2002.
With 74% of districts having already achieved elimination and only 29 districts (5%) having a PR of more than 2, progress toward achieving subnational elimination is well under way.
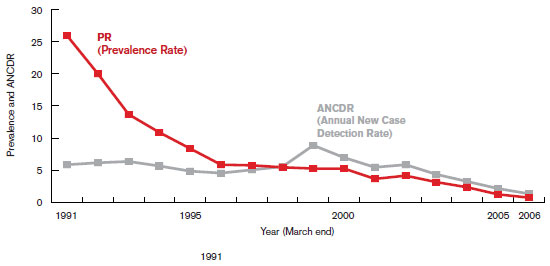
| Trend of Leprosy Prevalence & Annual New Case Detection Rates/10,000 Population |
Leprosy FACT
●India detected 161,457 new cases of leprosy during 2005, followed by Brazil (38,410), Indonesia (19,695) and the D.R. Congo (10,369) (WHO)
The face of leprosy in India will be hugely different from the past.
FUTURE STRATEGIES
For a few more years, India will follow the same strategy of case diagnosis and management through integrated services, continuous capacitybuilding of GHC staff, focused IEC activities, improved disability prevention and medical rehabilitation, and continuous monitoring and supervision.
In the current year, activities center on the following:
・continue efforts to achieve elimination of leprosy through existing MDT services in the remaining states/ Union Territories;
・focus attention on:
- endemic districts
- endemic urban localities
- districts showing high disability rates
- states with a high proportion of child cases;
・continue efforts to provide quality diagnostic and treatment services for leprosy in each peripheral health institution; provide services on all working days; underscore necessity for correct diagnosis by a PHC medical officer; continue process of validation by District Nucleus/District Technical Support Team; carry out proper counseling and case follow-up for better case-holding;
・improve capability of the GHC staff in prevention and management of leprosy disability, along with increasing the number of reconstructive surgery centers; plan for a three-tier system of prevention of disability services;
・continue capacity-efforts for all categories of staff whose involvement in the program is essential, both in rural as well as urban areas;
・continue to increase awareness about leprosy among the masses with the aim of bringing about attitudinal change and removing stigma against the disease;
・draw up a special activity plan for the year 2006-07 for the 29 districts remaining with a PR of more than 2/10,000.
| As awareness of leprosy increases, stigma diminishes |
LESSONS LEARNT
1. Repeated Modified Leprosy Elimination Campaigns (a total of five in eight years) with specific strategies for different areas helped detect nearly 0.99 million leprosy cases in a relatively short period of time (six days). Each successive MLEC showed detection of a much smaller number of cases, indicating that hidden cases were being flushed out and transmission potential reduced. New case detection dropped only after the 4th MLEC, which is very significant.
2. Mass awareness about leprosy was possible only through these campaigns organized at regular intervals. Interpersonal communication at village and community level has a big advantage over other IEC methods in NLEP.
3. Integration of leprosy services with the GHC system has helped patients a lot, not only because of increased accessibility but because of the confidence they gain from consulting with the Medical Officer. This creates greater acceptance and leads to more voluntary reporting.
4. The inexperience of GHC staff, the selfinterest of vertical leprosy staff and lack of patient awareness of the importance of completing treatment during the prescribed period caused certain “operational factors” to develop, which initially kept the leprosy case load higher than it actually was. Leprosy Elimination Monitoring surveys were carried out during the years 2002, 2003 and 2004 through independent agencies, which helped in pointing out deficiencies in the integrated system, availability of service in all health facilities, status of community awareness and operational factors.
Once these operational factors ― wrong diagnosis, re-registered cases, non-existent cases, non-release of patients from treatment even after completion, irregularity in drugs collection by patients, lack of follow-up ― were identified and corrected, the results were soon apparent.
Although the goal of leprosy elimination as a public health problem at the national level has been achieved, the government will continue with its program of leprosy eradication, to bring the benefits to people living in all parts of the country. There is no place for complacency at any level. The face of leprosy in India during the next six years is expected to be hugely different from the past.
|