|
COUNTRY REPORT
Lessons from Madagascar
The long and bumpy road to leprosy elimination
AUTHOR:
Dr. Vololoarinosinjatovo M. Monique
| Dr. Vololoarinosinjatovo M. Monique works for the National Leprosy Program, Madagascar. |
Madagascar achieved the goal of eliminating leprosy as a public health problem at the end of 2006. Having worked for the Leprosy Elimination Program since 1997, I would like to share some thoughts on the problems we faced and the lessons we have learned.
Following its inception in 1990, the program went through different stages. It began with the training of health workers and the dispatch of MDT and case-management tools to health centers. From 1997, new case detection/treatment activities were implemented, in the beginning focusing on high endemic areas. These activities started with a leprosy elimination campaign followed by special action projects, and were intensified in subsequent years.
As a result, the detection rate in 1997 was four times what it had been in 1996. Many new cases were detected, and many of them (around 60%) were correctly cured.
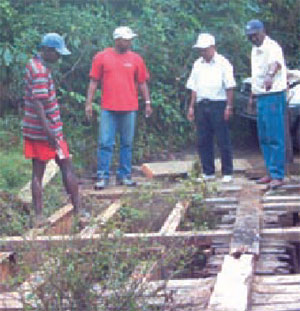
But after four or five years we noticed that the prevalence rate (PR) in some districts remained as high as ever. To check on this problem, we visited two remote, high endemic districts that had not been visited in many years. I will never forget one day-long journey of just 43 kilometers, during which we had to cross 84 damaged bridges, three-quarters of which had to be repaired with planks before we could get over them.
Through these two visits, we realized that there was a significant problem regarding the registration of leprosy cases at the peripheral level: cured patients were not being removed from the register, old cases were being registered as new cases, and patients were being wrongly diagnosed.
Obstacle en route to a remote district
The discovery also suggested that our data was probably flawed at every level, and that the problem needed to be urgently addressed because it might be one of the reasons why Madagascar's prevalence rate remained high.
We determined that the most effective way to resolve the situation was to carry out a diagnosis validation at the peripheral level followed by a register update. As a result of taking these steps, PR began to decrease. We called this period “our final sprint,” during which time we expended a lot of hard effort. On one trip to a remote health center to re-examine some leprosy patients, the motorcycles we were riding fell over three times because of the bad road conditions following the previous day's rain.
“On a journey of 43 kilometers, we had to cross 84 bridges, three-quarters needing repairs.”
SOME CONCLUSIONS
In the beginning, we didn't give enough training to peripheral health workers before sending them out on active detection, resulting in over or under diagnosis. In addition, we had to cope with staff turnover, although this was unavoidable. We were also too focused on new case detection, neglecting patient follow-up, to ensure that each patient was correctly cured.
Consequently, we had to clarify our epidemiological situation by introducing a new strategy of diagnosis validation followed by register update, something that could have been avoided had we focused on quality of service from the beginning.
Furthermore, by overly concentrating on the elimination goal, we neglected the human side of patient care, such as disability management and rehabilitation.
From these experiences I believe that leprosy control should focus on quality, not quantity. If we respect quality of service, then quantity will follow. Improving quality services is the best way to reach the goal of elimination.
Reaching the goal is not the end of the road, however. Considering the problem of under diagnosis, there are many new hidden cases to be detected and cured. The post-elimination period is even harder, and we must redouble our efforts and apply the lessons learned.
|