Myanmar provides an excellent example of how
effectively leprosy can be combated through a concerted
effort backed by the political will to achieve specific
goals. The overall effect of this effort has brought about
impressive results. There were many factors involved,
including medical technology, a resolute political will to
meet the challenge, effective networking of domestic
organizations, and support from overseas organizations.
More importantly, there was a shift on the front lines
from combating the disease only with specialists, to
treating it as a part of regular health care. This has
included the utilization of a nationwide network of
midwives who perform both an educational and medical
role in interacting with patients and their families.
Myanmar's success in dealing with leprosy is both
interesting and instructional as an effective model for
combating this disease wherever it continues to affect
people.
Isolation Era
The fight against leprosy has gone through
overlapping stages, including an Isolation Era which
began at the tail end of the 19th century and consisted of
the legal isolation of patients in colonies, where they were
not allowed to have any contact with society or even their
own families. On a smaller scale, some families built a
second small house near their main house, or had an
isolated room in their house as a means of isolating a
family member with leprosy. By the 1950s, Myanmar
was known to have one of the highest prevalence rates of
the disease, with the number of cases in 1951 estimated
to be fifty per ten thousand inhabitants, with 100,000
cases in the country as a whole.1
Vertical Era
Medical treatment began in 1952, when the drug
Dapsone was used in the Leprosy Control Program
begun with assistance from the World Health
Organization. During this period of time, the process
was mainly vertical, with patients solely interacting with
professionals. This interaction was somewhat effective
within its scope, but limited by resources and the finite
number of professionals, who were logistically unable to
operate on a larger scale. The drug itself proved to be of
limited effectiveness in the long run due to the
emergence of drug resistance to Dapsone, but
implementation of its use provided the beginnings of a
foundation for more effective ways of combating the
disease.
Integration Era
In 1969, the government of Myanmar made the
decision to better respond to patients' needs by beginning an expansion of Basic Health Services (BHS) into rural areas.
This killed two birds with one stone by integrating leprosy care into the program,
as well as enabling the utilization of midwives, who are able to supervise treatment
of existing leprosy patients during monthly visits to patients' homes and also
detect new cases. The midwives, as the health workers in closest contact with
patients in peripheral regions and already an integral part
of rural life, are more easily trusted than outside
specialists by many in remote regions. Wearing red skirts
and riding red bicycles, they are called "Red Angeles."
Red Angels at the GAEL Meeting
This shift to a nationwide horizontal network to
effectively spread life-saving information to the far
reaches of the country is an effective system for
combating other public health threats as well. In this
regard, the benefits of a horizontal network go far
beyond any single application.
Partnership Era
The roots of this era reach back five decades,2
culminating in a unified effort in recent years that has
lead to success through the cooperation and enthusiastic
efforts of many organizations - both local and
international, including help from WHO and UNICEF,
as well as logistical, technical and/or financial support
from several members of ILEP (International Federation
of Anti-Leprosy Associations), including the Sasakawa
Memorial Health Foundation.
According to a 1973 WHO Leprosy Assessment
Team survey, the leprosy prevalence rate was 239 per
10,000 inhabitants.
From early 1999, a general enlightenment of the
population regarding the true nature of leprosy has been
achieved in large measure due to the efforts of media personalities, who have provided invaluable assistance
with a comprehensive campaign consisting of more
component parts than it is possible to do justice to in this
article. This has included the work of more than 70
writers, whose material has been utilized in videos,
newspapers, periodicals and other print media. In
addition to print media, the message has also gone out
via television and radio, as well as through educational
meetings conducted by health workers and local NGOs
at events such as the "National Leprosy Elimination
Awareness Week."
As a side benefit to detection of new cases, leprosy
elimination campaigns have also resulted in significant
health education benefits. In 1978, the People's Health
Plan-I was implemented and, with the support of local
NGOs and community leaders in particular, has been a
major contributing factor in reducing the stigma of
leprosy. During this time, the number of registered
leprosy patients was at its peak, with nearly 270,000
cases.
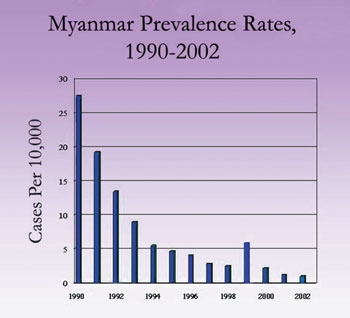
WHO recommended Multi-Drug Therapy (MDT)3
to Myanmar in 1986. At the time of implementation in
1988, the prevalence rate was 39.9 per 10,000 inhabitants. MDT was distributed on a limited basis
from the mid-eighties and then expanded to a
nationwide program, but still with limited coverage.
MDT services were integrated into BHS in the early
nineties, with full coverage being achieved in the late
nineties.
Special Ambassador Yohei Sasakawa visits a leprosy hospital in Myanmar
Triumph
By the end of 2002 there were only 5,494 cases under
treatment, with a rate of 1.04 per ten thousand inhabitants, and it has been announced that Myanmar
reached their leprosy elimination goal in January 2003
with a prevalence of less than 1 per 10,000 inhabitants.
The main challenges for the future are to eliminate
leprosy at the remaining divisional and township levels,
while simultaneously sustaining community awareness
and participation, as well as furthering improvement of
the quality of health workers to meet changing situations
and needs, including assisting with rehabilitation.
Continuous Improvement
One of the most important lessons that can be
learned from Myanmar's campaign has been the way
effective action has been built upon the lessons learned
from past results. Based on a cycle of plan, action, and
analysis, the result is carefully evaluated, shortcomings
noted, a new plan drawn up in response to those
shortcomings, and then a new cycle of plan, action, and
analysis begun. This type of focus on continuous
improvement is a universal strategy applicable to a
diversity of national settings.
Logistics Backed by Political Will
Presently, the total effect of all programs, combined
with the advances in medical technology represented by MDT and the infrastructure of the entire leprosy
elimination effort, have brought the prevalence rate
down dramatically. If there is one overall theme running
throughout the story of Myanmar's successful campaign
against leprosy, it could be said to be logistics backed by
political will. Naturally, the medical advances leading to
MDT were vitally important. However, the current
positive outcome could not have been achieved without
the coordinated efforts of so many groups and individuals
towards a common goal. This is perhaps the most
important thing for those of us with major battles ahead
to remember - that the focus of our efforts must be the
goal, and an ever-present searching vision that looks for
the proper logistical methods to achieve that goal.
In Myanmar, having now surpassed the official goal
of elimination, it is vital that complacency not set in, as
the need for a sustained effort must be maintained to
deal with future incidences of the disease. Community
awareness regarding the disease, self-diagnosis, and
treatment procurement, are all as important as ever,
underlining the importance of effective and accurate
education at every level of society.
Based on data obtained from Progress Towards Leprosy Elimination in
Myanmar, Ministry of Health, Myanmar, January 2003
1
According to WHO, elimination of leprosy as a public health problem has been defined since 1991 as a prevalence rate of less than one case per 10,000 in habitants.
2
For a detailed timeline, see Progress Towards Leprosy Elimination in Myanmar.
3
MDT - two to three drugs (Clofazimine, Rifampicin and Dapsone), which are used in combination to prevent resistance.